EXPANDING THE EFFECTIVE RANGE AND READINESS OF THE MEN AND WOMEN OF THE U.S. ARMED FORCES IS CRUCIAL AS FORCE SIZE IS BEING REDUCED
White Paper by
Richard C. Schnirring, PhD
Executive Summary:
February 23, 2014 (Washington)
“Defense Secretary Chuck Hagel plans to shrink the United States Army to its smallest force since before the WWII buildup ….” The Air Force, Navy, Marines and National Guard Units will also see drawdown in force. This makes in vitally important for our War Fighters to be ready for rapid deployment. And to be field ready our service men and women need to be physically fit to endure more time in the field, carry heavier loads, be quicker and stronger. However, studies show that members of the armed forces are predisposed to musculoskeletal injuries as a result of all the physical training and field duty preparation needed to achieve maximum force readiness. Musculoskeletal injuries include: ankle, foot, knee, hip, lower back and shoulders. Studies have concluded that the militaries current proactive use of OTC & custom orthotics effectively increases injury rates in basic training by 9%. 2007 DOD statistics show that these types of injuries were the second cause of hospitalizations and the leading cause of OP clinical visits. And the Bottom Line according to Economic Analysis of Information Management Requirements, Injury Cause Coding, March 2006: The total annual cost burden of these injuries is: $1,500,000,000 – yes $1.5 Trillion Dollars. According to Medical Surveillance Monthly Report, April Issue 2007, there are 900,000 injuries per year, affecting 675,000 service members which in effect is 50% of the military force annually. Musculoskeletal injuries accounted for 68% of all days of limited duty (DLD) which equates to approximately 25 million limited duty days per year. These injuries result in lost training time, increasing attrition rates and decrease in time in field and all are important in terms of force readiness. Inflammation and pain because of overuse/stress result in foot, knee, ankle, back and shoulder injuries. It is imperative to understand that the degradation of foot functionality and weakness leads to a predisposition to injury and reduced performance in the musculoskeletal system. Muscloskeletal alignment and balance begins with the feet or foundation. The loss of foot functionality and the resulting asymmetries and loss of balance are the main cause of a warriors’ loss of strength, stamina, speed, response time, injury and removal from field of duty; thereby reducing the effective range and readiness of the men and women of the U.S. Armed Forces. Patented science and technology exists that can help our war fighters achieve optimal physical fitness / readiness levels and prevent lower extremity injuries. This scientifically proven and patented technology provides the basis for a biomechanical product that actively stimulates , strengthens and restores the foot , balance and gait related musculature. All movement is related to balance. It has been determined since 1986 ( Shumway-Cook balance test) that the brain relies on sensory input from three areas to effectively manage its job of balance, posture and dynamic movement. The eyes, the inner ear and the feet. Without Barefoot Science or walking barefoot in the sand the soldier is left to compensate for a balance or proprioceptive deficit. Barefoot Science provides the soldier with the third leg of the balance tripod. Dr. Gorman (who invented the Microgate gait and balance system that the U.S. Military has standardized on in 300 locations) refers to this as being D.R.U.N.K. ( Dramatically Reduced Utilization of Norman Kinematics) Barefoot Science non orthotic inserts are designed to provide effects that are remedial, therapeutic and preventative – resulting in optimized foot health and foot functionality resulting in expanding the effective range and readiness of the men and women of our armed forces.
Proprioception The Body’s Built-In Injury Avoidance System
Proprioceptors are sensory receptors or nerve endings that relay information about motion , balance or position making us aware of our body position and movement in space. There are 400,000 proprioceptors in the feet that nourish the brain with sensory information. In addition to providing information about movement and balance they trigger certain protective reflexes without thinking.
The “Stretch Reflex” is activated when the proprioceptors sense too much stretch or force on a muscle or tendon that could lead to muscle or tendon injury. The reflex causes the stretched muscle or tendon to contract or shorten in a fraction of a second to automatically protect the structure. Olympic Coaches have commented that BFS has reduced their athlete’s ankle and tendon sprains by 50% due to this natural injury prevention gift.
Introduction and Problem Definition:
“A progressive, silent, seemingly unimportant foe has emerged as the number one health threat to U.S. Armed Forces. This threat is caused neither by virus or germ, but by a military tradition to perform, excel and exceed. Its name is INJURY – and it represents the greatest threat to U.S. Military READINESS”
Major Vancil McNulty, Physical Therapy Staff Officer
U.S. Army Center for Health Promotion and Preventive Medicine
Army Medicine: August 2009
According to (USARIEM) – MIL MED, 2011 reported that the rates of ankle and foot injuries in active duty U.S. Army Soldiers (ADA) studied between 2000-2006 are a major cause of active duty time lost from training and combat operations. 16% of all soldiers were clinically seen at least once for an Ankle / Foot Injury (AFI) and 60%-70% of ADA soldiers with AFI had ankle sprain / strain. An AFI history in the previous 2 years increased the AFI rates by 93% to 160%. It was recommended by the authors that “these groups should be targeted for preventive medicine”.
According to Medical Surveillance Monthly Report, April Issue 2007, there are 900,000 injuries per year, affecting 675,000 service members which in effect is 50% of the military force annually. Musculoskeletal injuries accounted for 68% of all days of limited duty which equates to approximately 25 million limited duty days per year.
COST BURDEN OF MUSCULOSKELETAL INJURIES: U.S. Army Lt. Col. Deydre Teyhen from Fort Detrick: (Army Only 2013) reported that musculoskeletal injuries resulted in about 2.4 million medical visits to military treatment facilities and $548 Million in direct patient care costs. Lt. Col. Teyhen went on to say that 73% of VA disability claims include a musculoskeletal component.
The bottom line is that the total average cost per injury is over $3000.00, THE TOTAL ANNUAL MILITARY COST OF INJURIES IS: $1,500,000,000 ($1.5 TRILLION). (Source: Economic Analysis of Information Management Requirements, Injury Cause Coding, March 2006) – An important question would be: What percentage of these injuries is preventable?
Members of our U.S. Armed Forces should be considered and treated as world class athletes. Dr. James Onate, Assistant Professor of Exercise Science and Director of Old Dominion University Sports Medicine Research Lab was quoted in Military Sports Medicine: Quest Summer 2004 as saying: “We expect highly paid athletes to be in outstanding physical shape and to have the best sports medical care possible when they step on to their field of battle, but; what about our country’s true soldier? How are we helping our military athletes achieve optimal physical fitness levels and prevent injuries while keeping them in the most important game of all – protecting our Country?” Dr. Onate is addressing optimal force readiness.
2007 DOD statistics show there were 2.1 million injury related medical visits, affecting 900,000 service members. Injuries were the second cause of hospitalizations, accounting for almost 110,000 days as in patients. Injuries were, and are, the leading cause of outpatient visits. Musculoskeletal injures accounted for 68% of all days of limited duty and medical profiles: they add up to an estimated 25 million days of limited duty per year! The medical cost alone for 900,000 injuries is estimated at $700 Million. What % can be prevented? (Does not include cost of: DLD, LDD, LTD)
Military Sports Medicine: Quest Summer 2004 also reported that in 1999 the DOD listed military training related injuries as the leading causes of disability, decreased military readiness and lost productivity. In Operation Desert Shield & Operation Desert Storm, musculoskeletal injuries sustained OFF DUTY while participating in sports and recreational activities, as well as during physical fitness programs, were the leading cause of medical evacuations and hospitalizations. This article also points out that the Department of Veterans Affairs spends approximately $13 Billion and the Armed Forces pay $1.5 Billion annually to treat soldiers with disabilities caused by unintentional injury. Musculoskeletal and Orthopedic related injures account for 63% of all disabilities.
Navy Example – Musculoskeletal Injury Impact: In the Hampton roads area in Norfolk alone, 2000 Sailors were med boarded due to musculoskeletal injury. These medical boards were for the fleet only and did not include any shore based sailors. The loss of 2000 sailors is equivalent to losing 6 LHA’s OR LHD’s (amphibious assault ships). Or: 2000 sailors out of action = 6 destroyers unmanned!!
According to the Journal of Athletic Training: Jan-Feb 2010: ankle sprains have been reported as one of the most common injuries sustained by members of the U.S. Armed Forces. The incidence of ankle sprains among service members was 5 times greater than reported in civilian population studies.
Absolute and Relative Morbidity Burdens Attributable to Various Illnesses and Injuries, U.S. Armed Forces: MSMR, VOL 19, #4, April, 2012 reported that In 2011 taking ALL MEDICAL ENCOUNTERS and ALL SERVICES into consideration:
Knee encounters ranked 5th and bed days ranked 31st
Foot and ankle encounters ranked 10th and bed days ranked 16th
Leg encounters ranked 18th and bed days ranked 10th
According to a military report in April 2011: “Musculoskeletal and connective tissue disorders & injuries accounted for almost 65% of all limited duty dispositions.
The American Journal of Preventive Medicine reported the following military injury results for Army, Air Force, Marines and Navy:
“There were 743,547 injury-related musculoskeletal conditions in 2006 (outpatient and inpatient, combined), including primary and non-primary diagnoses. In the report, 82% of injury related musculoskeletal conditions were classified as inflammation/pain (overuse), followed by joint derangements (15%) and stress fractures (2%). The knee/lower leg (22%), lumbar spine (20%), and ankle/foot (13%) were leading body region categories.”

The chart matrix above shows that lower extremity injuries account for 190,351 injuries or 39% of all injury related musculoskeletal conditions for all service branches.
The chart below breaks down the lower extremity injuries listed above into three areas. The knee, lower leg, ankle and foot injuries account for the majority of the lower extremity injuries. Lower extremity overuse injuries associated with running, marching and other lower extremity load bearing activities accounted for up to 75% of injuries among men and 78% of injuries among women during Army basic training.

The injury data available may differ slightly from source to source but the data undeniably shows that lower extremity injuries have a significant negative impact on force readiness. What is not being addressed is the need for lower extremity injury preventive measures and the cost burden caused by these injuries. Our service members are all predisposed to lower extremity injuries that start in basic training. They are issued “standard” footwear and are required to meet physical standards (marching, running, obstacle courses, climbing, exercising, jumping, fighting, carrying heavy loads and negotiate rough terrain). It is imperative that we understand that the degradation of foot functionality and weakness leads to a predisposition to injury and reduced performance in the foot, ankle, knees, hips, lower back and upper back and shoulders. This loss of foot functionality and degradation in neuromuscular feedback will lead to the warriors’ loss of strength, stamina, speed, response time, injury and removal from field of duty and training
One of the most compelling and definitely the most current report and featured article from the Journal of Special Operations Medicine – February 28, 2014 – issue 22: The summary of this article states that the number of musculoskeletal injuries increases in association with stress factors and that field commanders may conduct simple field tests is assess physical limitations but continues and (see full article below) specifically states in no uncertain terms that: “countermeasures for these KNOWN decrements are lacking in the scientific literature …”. And to bring these matters to their most intense and important level: “These countermeasures could prevent mission mishaps and may save the lives of Operators during severe operational stress.”

In 1996, Sherman, et al wrote: Prevention of Lower Limb Pain in Soldiers Using Shock Absorbing Orthotic Inserts. Sherman and his team read two studies that determined that lower extremity injuries were common during basic training and wanted to see if preventive measures could be taken. The article hypothesized that the use of “shock absorbing inserts” placed in the boots and sneakers of selected army basic trainees would result in less foot related problems than the trainees that were not issued the inserts. So, every other training unit was issued inserts prior to the start of training when boots and sneakers were fitted. 517 trainees were issued inserts, 397 were followed but not issued inserts and 218 were not issued inserts but purchased them on their own. According to post training questionnaires and the trainees’ medical records, the inserts did not have any preventive effect on occurrence of lower limb problems during training. Their results showed that 38% of those issued inserts had lower limb pain problems compared with 29% of those not issued inserts and 38% of those who bought their own. In summary: there was no statistical or practical difference between these rates of occurrence. The use of shock absorbing inserts did not have any preventive effect on occurrence of lower limb problems and physical fitness test scores and graduation rates were not affected. However, when the results of two different preventive studies of two types of inserts were compared there was a significant difference – so it was demonstrated that insert designs do work differently.
Science and Technology:
Professionals at all levels: drill instructors, special op members, athletes, coaches, trainers and therapists refer to the body as a complex machine. Barefoot Science (BFS) has developed a patented disruptive technology in the life sciences sector. This technology provides the basis for a range of innovative biomechanics products that actively stimulate, strengthen and restore the feet and gait related musculature to provide effects that are remedial, therapeutic and preventative.
BFS is a progressive approach that is in line with athletic training programs in that muscles are constantly and gradually challenged producing an improvement in the strengthening of the muscles. The patented BFS dome technology is strategically shaped and located to interact with the key region of the foot. This region corresponds with the foots center of mass, the location of the body’s line of action through the foot, the apex of the foot radiating arches and the nerve engorged plantar aspect of the foot.
Clinical evidence has shown that:
- BFS increases arch height which results in more even force distribution across the joints of the foot and a decreased tension on the plantar connective tissue – 44% increase in balance and stability.
- The morphological changes created through the use of BFS are a result of increased muscle contribution & contractions that create energy and motion. 36% average reduction in plantar surface area reported in 100% of subjects.
- BFS capitalizes on the mechanical properties of proprioceptive and neuromuscular areas of the foot as well as the neuromuscular properties of the sole. These properties influence reflex responses, sensory feedback of terrain and reduce predisposition to injury.
- Data collection and observations using sEMG monitoring and recording show
- Evidence of improvement in balance and stability.
- Evidence of improvement in pressure distribution, posture and gait
- More robust contraction patterns across all monitored muscles
- Increased performance ( reported in all cases)
The globally patented Barefoot Science Arch Strengthening System enables the wearer to strengthen the muscles and tendons of the entire foot and ankle complex. Who is using Barefoot Science? Olympic Gold medal Athletes, Gold Medal Firefighter Combat champions, FIFA coaches and athletes, the world’s most recognized Triathlete, Ultramarathon, U.S. Air Forces runners , cyclists and coaches, NFL players, Special Ops members, VA hospital, Walter Reed Hospital and men and women of all branches of the military are wearing the BFS foot strengthening system.
Testimonials and Clinical Evidence:
“(BFS is) Comfortable and ideal for balanced strength development … superior to anything out there.”
“I started working with Barefoot Science a few years ago and it has really turned our practice into a healing clinic”
Michael Olden, CPED, Triple Board Certified Pedorthist
This season “We didn’t have a single case of plantar fasciitis. We also didn’t have complaints for Achilles tendon pain. We saw a two inch improvement in vertical jump with Smart Jump (Fusin Sport) after our athletes train wearing Barefoot for only one day.”
Kostas Chatzichristo Med, CSCS
Trainer to the Greek National Basketball Team
Barefoot Science technologies clearly offer the most effective preventative and rehabilitative treatment option available today to address poor structural integrity of the foots arch system. I recommend it for cases of foot fractures and treatment above the ankle including knee, hip and lower back.”
Thomas D. McClain MD, ABOS, AAOS
American Board of Orthopedic Surgeons
“Barefoot Science has put together a very thoroughly researched Medical Overview. It has solid scientific evidence that supports the strengthening and functional adaption process. This direction follows closely to the chiropractic philosophy of restoring normal function. You will realize change throughout the entire Lower Kinetic chain.”
Dr. Lawrence Bell DC, FCCSSI © FICC ART
Professor
Once one understands and accepts the premise of foot dysfunction as the cause of non-traumatic pain patterns of the weight bearing structure, the logic behind Barefoot Science,as a therapeutic agent becomes crystal clear.”
Bruce Comstock DC
Author, Weight Training Safely
“I really like this product. I’ve been using it in my practice and it is a significant improvement over existing methods.” Tiffany Bourquet – Physiotherapist
“As an athletic development coach who works with professional athletes on a daily basis, the BFS system has become the greatest tool to have at my disposal for strengthening the lower extremity musculature. It’s been especially helpful in correcting muscle imbalances that might negatively affect foot strike patterns in gait as well as strengthening and stretching the ankle and foot following an injury.” Gray Cook – One of North America’s top fitness trainer.
“BFS is as easy to use as simply putting on your shoes. It has produced noticeable improvements in my overall speed, vertical jump as well as first step explosiveness.” Gerry Rush – Soccer Player, Canada
“Foot and ankle injuries are a huge problem in professional and amateur sports. BFS is the only product out there that allows for complete foot and ankle strengthening.” Scott Forehan – Worldwide recognized Muscle strengthening specialist.
In an independent third party study conducted in a clinical environment over 96% of the ER doctors and nurses reported pain reduction in at least one of 8 body parts studied. Overall pain reduction score for all 8 body parts was 83.3%. Overall reduction in fatigue was -22.7%. (See chart below for all data)
What does this mean to a runner?
Conclusion
David M. Lemke, NMT, sEMG Tech.
The hamstrings and gluteals are the big guns in running - and running is integral to
nearly all sports. My observations indicate:
- Improved muscle load distribution (evidence of improved participation of all
necessary muscles)
- Decreased asymmetrical inefficiency (evidence of shift toward L/R balance in
amplitude)
- Reduced fatigue (evidence of delayed onset)
- Decreased pelvic torsion + improved pelvic level = Core Stability
- Increased Performance (reported in all cases)
The Barefoot Science people know their insoles work - they've done extensive trials that show dramatic pain relief and improved energy. But I honestly don't think they realize how truly remarkable a product they've invented. These insoles help so many people with such a variety of complaints - not just because they align posture or provide cushioning and support for feet (like orthotics) - but because they activate the plantar musculature and foot bed proprioception which I believe. I believe it literally completes the upright posture circuit and brings about posture without effort!
Submitted by David M. Lemke, NMT, sEMG Tech
November 8, 2012
A study performed by New Balance Athletic Footwear on 458 adult subjects and members of their running clubs was conducted. The results showed that 97% of the users would continue to use the BFS product. 20% reported an increase in strength and 32% reported an increase in support.
A study conducted Huddersfield England showed when comparing the pre and post underfoot “surface area it was found that on average there was a 36.36% reduction in surface area. 100% of the subjects showed a reduction in plantar surface area.” 100% of subjects had their flat foot syndrome eliminated.
A study conducted by Scholl Japan showed that 58% of users rated their experience as positive, 55% perceived a reduction in pain and 56% reported an increase in their ability to walk with reduced pain or discomfort.
Mission Statement:
The U.S. Military spends a lot of time and money on developing protective / shielding devices to protect the men and women of our Armed Forces. Millions and millions of dollars are spent on developing safer vehicles, protective vests, eyewear and helmets. However, how much protective effort is being placed on the basic of basics: “Boots on the Ground!” What are we doing to protect and strengthen what gets our war fighters in and out of harms way? The feet! Barefoot Science inserts are ideal for all members of our armed forces. BFS provides protection, strengthening, alignment and efficiency for the foot and all gait related musculature. BFS will help the soldier eliminate their hidden deficits so they can stop training the compensatory system. This will give soldiers a gain in strength, balance, symmetry, stamina, speed, response time, decrease in injuries and the ability to remain longer and stronger on the field of duty. BFS provides the service men and women the advantage to develop and maintain high levels of physical fitness for the physically demanding duties they routinely perform. Stronger foot muscles help to ensure a proper stabilization of the foot. This ensures a better positioning of the foot beneath the body and better ensures proper alignment which increases the effectiveness and performance of the system and reducing injury. And most importantly as stated in the JSOM: “…these countermeasures could prevent mission mishaps and may save the lives of Operators during severe operational stress.”
BOTTOM LINE – COST BURDEN OF INJURIES – TOTAL ANNUAL COST = $1.5 TRILLION
Total cost savings given injury reduction of 5%: $75,000,000
Total cost savings given injury reduction of 15%: $225,000,000
Total cost savings given injury reduction of 30%: $450,000,000
Barefoot Science International Inc.
www.barefoot-science.com
1-877-651-3668
-Elimination of Flat Feet
- Symmetrical Foot to Shoulder Alignment
-
Prevents Injury


]]>























 We have learned that barefoot walking in sand improves proprioception due to mid arch stimulation. However not everyone has the opportunity to walk in the sand barefoot 24/7. Luckily, there are products that claim to help this fact.
We have learned that barefoot walking in sand improves proprioception due to mid arch stimulation. However not everyone has the opportunity to walk in the sand barefoot 24/7. Luckily, there are products that claim to help this fact.  All of these factors lead to the fact that the foot is no longer healthy and capable of being self-supportive.
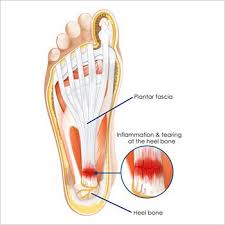
All of these factors lead to the fact that the foot is no longer healthy and capable of being self-supportive. Heel spurs can easily be prevented and treated through the use of the BAREFOOTSCIENCE™ Strengthening System. The Barefoot Science insoles help to ease the tension and strain placed on the plantar fascia which heal the damaged tissues and prevent a recurrence of the problem. The insoles allow the arch to stabilize naturally, keeping the heel spur parallel to the ground, and less likely to protrude into surrounding tissue.
Heel spurs can easily be prevented and treated through the use of the BAREFOOTSCIENCE™ Strengthening System. The Barefoot Science insoles help to ease the tension and strain placed on the plantar fascia which heal the damaged tissues and prevent a recurrence of the problem. The insoles allow the arch to stabilize naturally, keeping the heel spur parallel to the ground, and less likely to protrude into surrounding tissue.





 Common symptoms of back pain include lower back muscles cramping; muscle spasms with associated discomfort in the gluteal region; and pain in the lumbar spine.Back pain too can result from a number of different factors such as: muscle or ligament strains; bulging or ruptured discs, arthritis, skeletal irregularities; nerve-related pain caused by irritated or pinched nerves; and osteoporosis.
Common symptoms of back pain include lower back muscles cramping; muscle spasms with associated discomfort in the gluteal region; and pain in the lumbar spine.Back pain too can result from a number of different factors such as: muscle or ligament strains; bulging or ruptured discs, arthritis, skeletal irregularities; nerve-related pain caused by irritated or pinched nerves; and osteoporosis.{kind=link}